Premium content
Access to this content requires a subscription. You must be a premium user to view this content.

Would you like to see your presentation here, made available to a global audience of researchers?
Add your own presentation or have us affordably record your next conference.
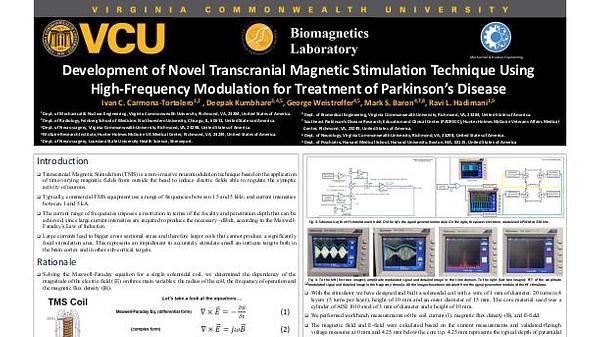
Introduction: Transcranial Magnetic Stimulation (TMS) is a neuromodulation technique currently FDA approved to treat depression, migraine and obsessive-compulsive
disorder (OCD). TMS outcomes are known to vary based on individual neuroanatomy, tractography derived structural connectivity, and functional connectivity which is not well
understood 1,2. There is a disconnection between what is measured empirically in resting motor threshold (RMT)/treatment outcomes, and computer simulated induced electric fields (EField)
values based on Magnetic Resonance Imaging (MRI) derived head models. In this study, we aim to gain an understanding and explanation of this variability and offer an
improvement by taking region of interest (ROI) specific gray matter (GMV) and white matter volume (WMV) over a previously published relationship between the brain scalp distance
(BSD) and E-Field in the Transcranial Magnetic Stimulation (TMS).
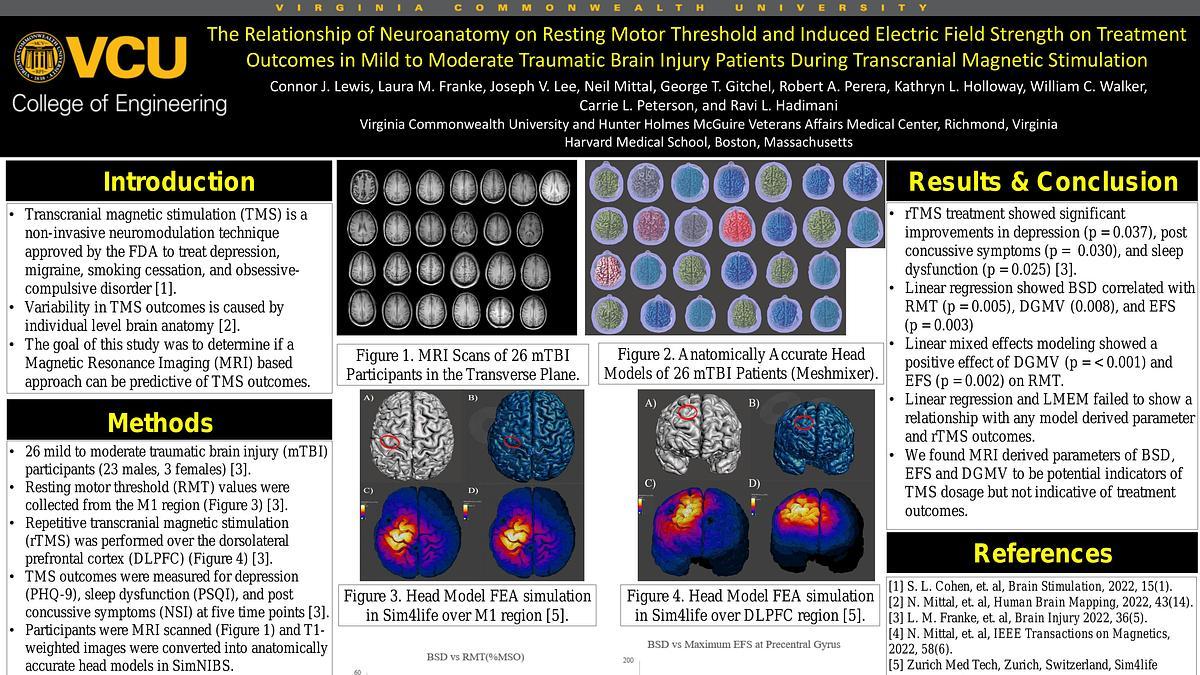
Experimental Details: Twenty-six mild-to-moderate traumatic brain injury (mTBI) patients were recruited as described in our previous publication 3. Participants underwent MRI scans
followed by guided repetitive TMS using a NextStim NBS4 figure-of-eight double coil. RMTs were taken as a percentage of the maximum stimulator output (%MSO). T1 weighted MRI
images went through SimNIBS pipeline (v3.2.6) to create anatomically accurate head models for each patient. Head models were imported into Meshmixer (v3.5) where BSD and
individual segment volume were taken from the precentral gyrus (knob) as described in 4.
Results: Preliminary analysis indicates a weak but negative correlation between both GMV (R2 = 0.0307, p = 0.392) and WMV (R2 = 0.0388, p = 0.335) versus RMT. And a stronger
positive correlation between BSD (R2 = 0.29, p = 0.0046) and RMT.
Conclusion: Segmented ROI brain volume didn’t improve the correlation between RMT and 3D brain-scalp volume compared to RMT and 1D brain-scalp distance. Further investigations
into E-Field and correlating empirically collected patient outcomes will enable better TMS dosages as a percentage of patient specific RMT for TMS procedures.
References:
1 T. Herbsman, L. Forster, C. Molnar, et al., Human Brain Mapping., 30(7), 2044-2055 (2009). Motor threshold in transcranial magnetic stimulation: the impact of white
matter fiber orientation and skull-to-cortex distance.
2 N. Mittal, B. Thakkar, C. B. Hodges, C. Lewis, Y. Cho, R. L. Hadimani, & C. L. Peterson, Human Brain Mapping, 1-16 (2022). Effect of neuroanatomy on corticomotor excitability
during and after transcranial magnetic stimulation and intermittent theta burst stimulation.
3 L. M. Franke, G. T. Gitchel, R. A. Perera, R. L. Hadimani, K. L. Holloway & W. C. Walker, Brain Injurty, 36:5, p. 683-692, (2022) Randomized trial of rTMS in traumatic brain injury:
improved subjective neurobehavioral symptoms and increases in EEG delta activity.
4 T. A. Yousry, U. D. Schmid, H. Alkadhi, D. Schmidt, A. Peraud, A. Buettner, P. Winkler, Brain, Vol. 120, p.141-157 (1997) Localization of the motor hand area to a knob on the
precentral gyrus. A new landmark.